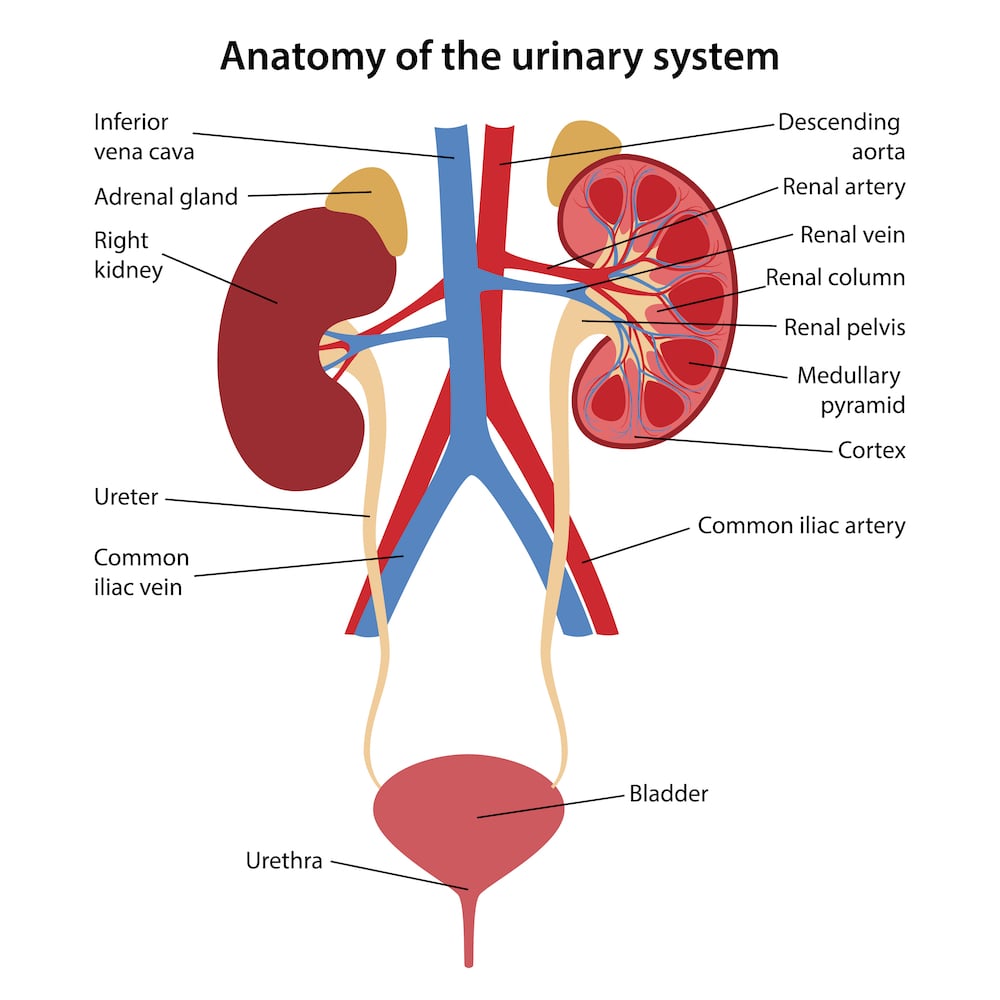
The ureters are a part of the genitourinary tract, and they are found on both sides of the body. They are long, hollow, and thin tubes that help to drain urine from the kidneys into the bladder. Sometimes, there may be some dysfunction in the ureter, which may warrant the need for medical or surgical management.
Who would need to undergo reconstructive ureter surgery?
A patient may need to undergo reconstructive ureter surgery in the event that the ureter has been damaged by trauma or inflammation. When the damage heals, a scar may form, resulting in an area of narrowing (called a stricture) at the ureter.
Treatments
Ureteric anastomosis / reimplantation
Ureteric anastomosis involves joining two ends of the ureter after a segment of it has been removed. It is often done in cases where there is ureteral injury and subsequent stricture formation. The type of surgery required is dependent on the site and length of the stricture. The aim is to achieve a water-tight and tension-free anastomosis.
Ureteroureterostomy
A ureteroureterostomy is usually performed when there is a short segment stricture at the upper or mid ureter. The narrowed or stricture segment is excised, and the two ends of the remnant ureter are widened and anastomosed together. This surgery can be done via open surgery, laparoscopic or robotic surgery.
Transureteroureterostomy
Image taken from abdominalkey.com
A transureteroureterostomy, on the other hand, is indicated when a longer segment of the distal ureter is obliterated or not suitable for repair. The involved ureter is cut above the level of the stricture, and the remnant portion is brought across to the opposite side and connected to the healthy ureter on the opposite side.
Ureteral Reimplantation
Ureteral reimplantation is usually performed for distal ureteric strictures. The involved ureter is joined directly to the bladder (uretero-neocystostomy) in a refluxing or non-refluxing manner. If the gap between the ureter to be reimplanted and the bladder is too wide, other procedures such as a psoas hitch or a Boari flap can be performed to bridge the gap.
Ileal Interposition Graft
This surgery is performed when an extremely long segment of the ureter is injured. A segment of the small intestine, usually the terminal ileum, is used to connect the involved remnant ureter or kidney to the bladder.
What to expect
Before the surgery, you will first meet with a urologist who will discuss your surgical options with you, take a detailed medical history and perform a physical examination. Some investigations may also be done to assess your kidney function and bladder function.
You will also have an appointment with the anaesthetist, a doctor in charge of administering anaesthesia to you during the surgery. The anaesthetist will take a further look at your medical history and background to assess your fitness and suitability for the operation, as well as give you advice on what you can and cannot do before the operation and what medications you should stop before the procedure. For example, patients are advised to stop blood thinners before the operation to reduce the risk of excessive bleeding.
UU and TUU are both done under general anaesthesia and may be done either via open surgery involving a large vertical incision through the centre of the abdomen, or via minimally invasive methods such as robotic surgery or laparoscopic surgery.
During the surgery, before the two ureter ends are joined together and sutured, a stent will be placed into the ureter to ensure that the lumen does not collapse onto itself and to ensure that the ureter remains patent after healing. A urinary catheter will also be inserted to help drain urine out of the bladder.
After the procedure, the ureter stent will be removed about one month later, and radiological imaging will be done periodically at follow-up appointments to help to check for any abnormalities in the kidneys and ureter and for any obstruction and dilatation.
Ileal conduit
The creation of an ileal conduit involves surgically fashioning a tube from a piece of the small intestine (most often the ileum) to attach to the ureters and kidneys to allow urine to drain out of the body. The urine will then exit the body through a small opening in the skin, known as a stoma. After the surgery, the person will live with a urostomy bag that collects urine.
Who is an ileal conduit procedure recommended for?
An ileal conduit is the most common form of urinary diversion performed by urologists to resume continuity of the urinary tract after a patient undergoes a surgical procedure to remove the bladder. The ileum serves as an alternative pathway for the drainage of urine from the kidneys out of the body. Surgeries to remove the bladder are most often indicated in cases of cancer.
What to expect
The surgery can either be done via the traditional, open surgery method (which involves a long cut down the centre of the abdomen) or through minimally invasive surgery, which involves either the use of robotic surgery or laparoscopic surgery.
Similar to the aforementioned condition, a urology referral and check-up, as well as an appointment with the anaesthetist, will be conducted before the surgery.
The urologist will take a closer look at your medical history, and if you have cancer, they will also discuss at length with you the treatment options that are available. Because ileal conduits are often part of a major surgery, other surgeons, like a colorectal surgeon, may also be involved in the operation. You will be given advice on what medications to take and stop, what lifestyle measures to institute before the operation, as well as be given more information regarding the ileal conduit surgery.
Maintaining the ileal conduit will be a routine part of your everyday life. You will be briefed on how to look after your stoma properly. It is also important to help maintain your overall health after the surgery.
Summary
Ureter reconstructive surgery is a good surgical option when there is damage sustained to the ureters as a result of trauma and malignancy. If you are a candidate for such surgeries, do be sure to make an appointment to explore your treatment and surgical options.